Therapist SEO: Why Search Volume Is the Wrong Metric
The most common pattern we see in first audits: a therapist who treats complex PTSD, attachment trauma, or OCD has twelve blog posts explaining what anxiety is — and zero pages about their actual specialty. The high-volume content they spent months writing is unranked, unbookable, and competing against WebMD.
In mental health SEO, the keywords with the most searches are often the worst investments for a private practice. Not because of bad writing, but because of structural forces that generic SEO tools were never built to account for.
At Koppla, every content recommendation starts with a multi-factor evaluation, one that looks nothing like a standard keyword report. Here's what it actually measures, and why it's built the way it is.
TL;DR
Before we recommend a single content topic to a therapy client, we evaluate it across five distinct dimensions. None of them is search volume. This post explains why that matters — and walks through exactly what we measure instead. Hint: It's a bit of math, a lot of SERP (Search Engine Results Page) analysis, and a deep understanding of how mental health search works in practice. We have built this framework into our Site Performance page on KopplaHQ.
Why Mental Health SEO Is Fundamentally Different
Generic SEO logic fails mental health practices for reasons that are specific to how Google treats this category. The structural forces at play here don't exist in e-commerce, SaaS, or local services.
The YMYL Problem
Google classifies mental health content as YMYL — Your Money or Your Life — its strictest quality tier. This designation means Google applies heightened scrutiny to who is publishing the content, not just what the content says.
The practical consequence is that generic blog content from practices without demonstrable clinical authorship is actively suppressed in favor of sources with institutional or medical authority. When you write about depression, you are not competing with other therapist websites. You are competing with Mayo Clinic, WebMD, the National Institute of Mental Health, and the American Psychiatric Association.
That is not a fight a single-location private practice can win on general clinical definitions. There is terrain in mental health search where a credentialed local clinician has a structural advantage that no national publisher can replicate. Our framework is designed to find it.
The Crisis SERP Phenomenon
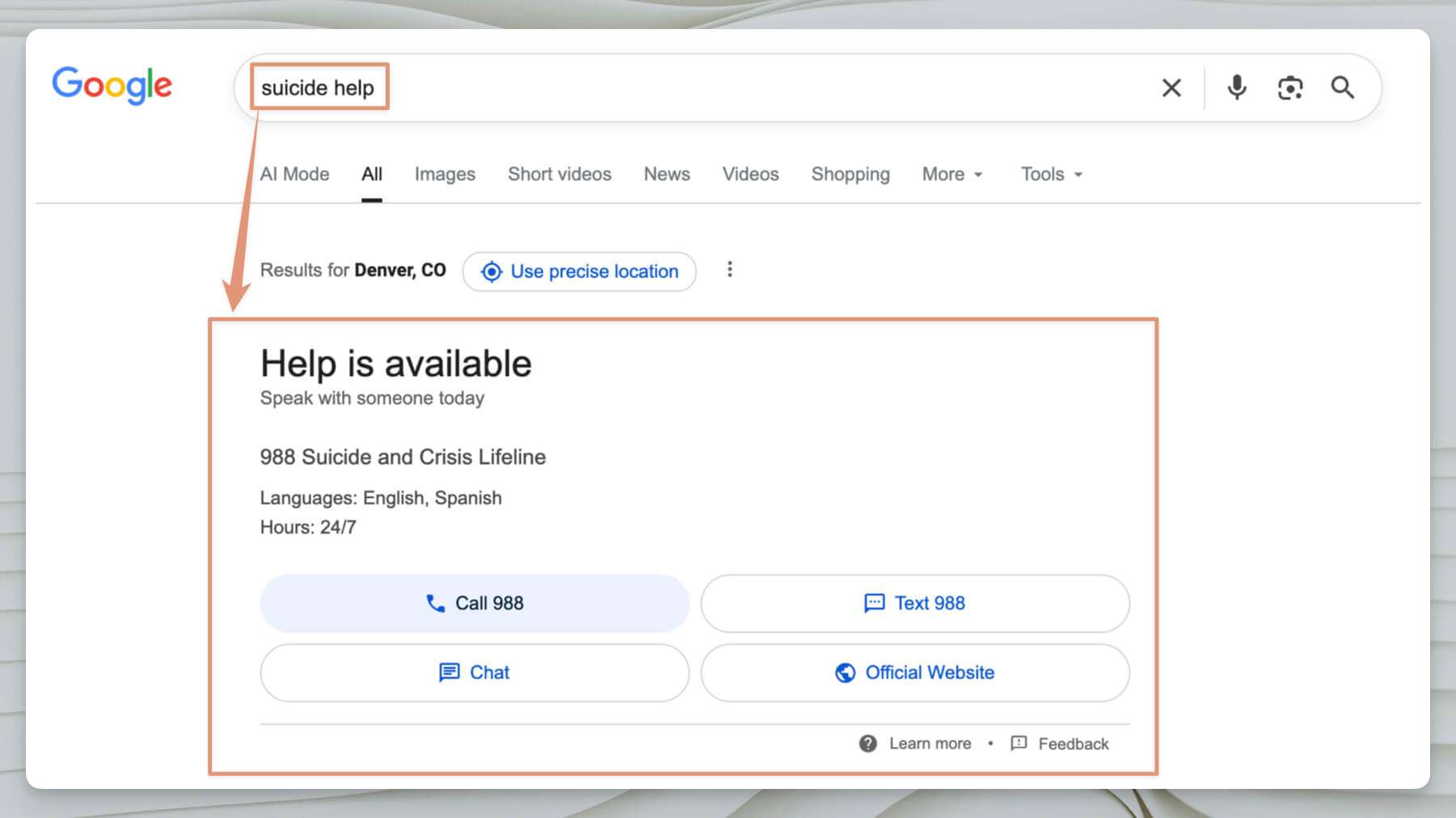
For many high-volume mental health searches — anything touching suicide, self-harm, or acute mental health crises — Google inserts the 988 Suicide & Crisis Lifeline box above all organic results. This is not a ranking problem. You can rank #1 organically and still capture near-zero clicks because the SERP's above-the-fold real estate belongs entirely to the crisis intervention feature.
Most SEO agencies don't know this exists. It isn't a factor they track, because it doesn't exist in any other industry they work in.
The AI Overview Collapse
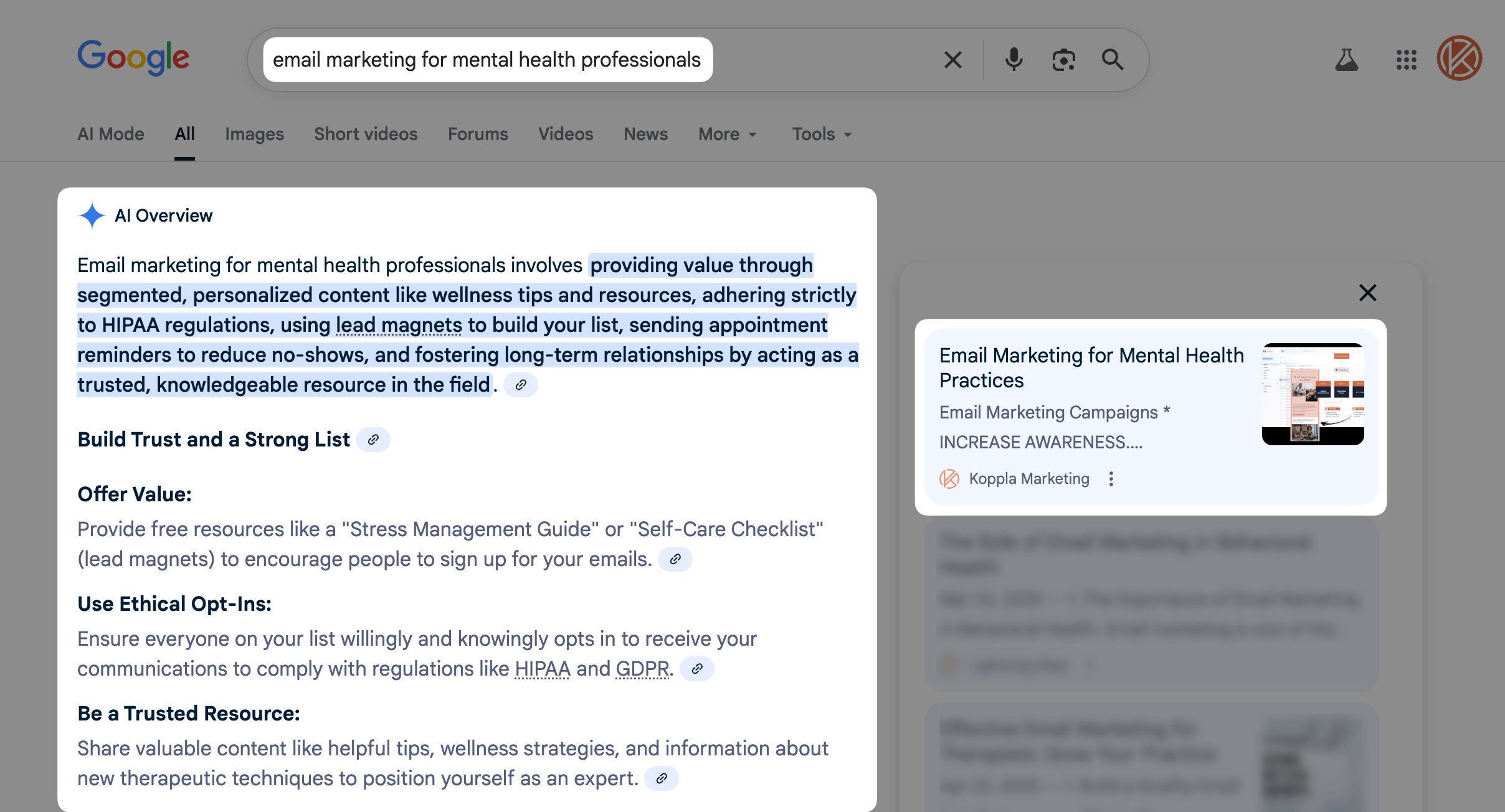
As of 2025–2026, AI Overviews are a serious headwind. Industry research shows they suppress organic click-through rates by more than 60% on informational queries, a pattern we see consistently in mental health search. The mechanism is straightforward: Google answers the question in the AI Overview panel directly, eliminating the user's need to click through to any webpage.
So this begs the question, What kind of queries trigger AI Overviews most reliably?
Informational ones.
Exactly the "What is anxiety?" and "Signs of depression" and "Trauma therapy approaches" content that makes up the majority of most therapist blog strategies. The vast majority of AI Overview triggers are informational queries, which happens to be where most therapy content budgets go. This pattern is especially pronounced in mental health search. The most common trigger for AI Overviews is general condition definition content.
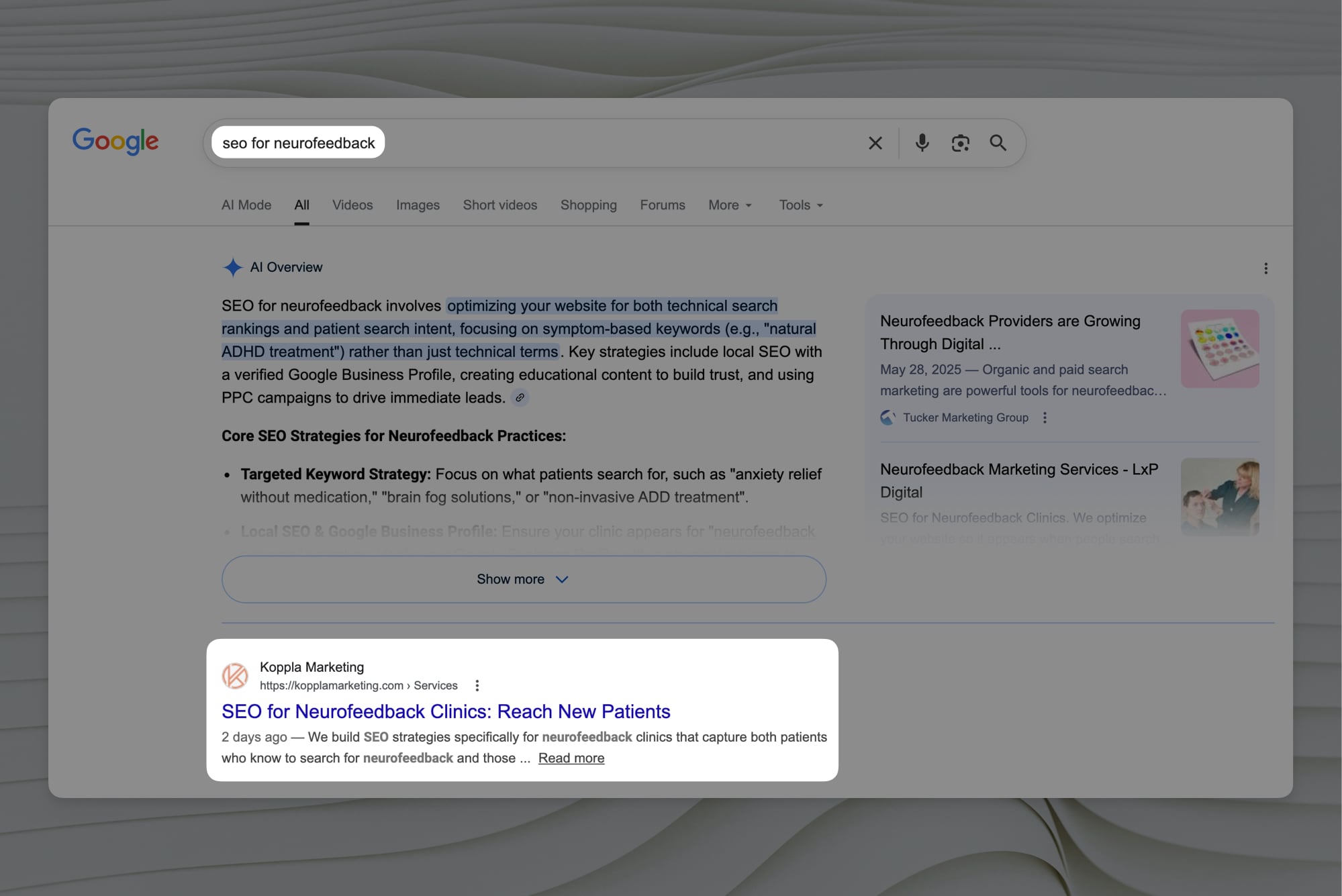
This doesn't mean informational content has no place in your strategy. It means the ROI calculation for informational content has changed dramatically, and the way most agencies still sell it has not caught up. Our framework accounts for this by evaluating the SERP for AI Overview presence before recommending any informational content, and deprioritizing it when the click-through suppression is severe.
The Directory Wall
Broad searches for therapy — "therapists near me," "anxiety counseling," "therapist in city" — are dominated by healthcare directories and aggregator websites. These directories have massive domain authority, extensive backlink profiles, and years of established trust signals. Outranking them on general terms is not a realistic goal for a single-location private practice with a standard marketing budget.
But directories have a critical weakness: their content is generic by design. They cannot write a specific, clinically expert page about treating obsessive-compulsive disorder in software engineers in Seattle. A therapist who specializes in exactly that can win on that particular topic in the search engines. The problem is that most practices don't know to look for these specific niches, and most agencies don't know how to find them.
The Five Dimensions We Actually Evaluate
General SEO tools were designed to answer one question: how many people search for this, and how hard is it to rank? That's a useful starting point for an e-commerce store. It's an insufficient and often misleading framework for a private practice marketing to a local, specialized, high-stakes audience.
Before we recommend a single content topic to a therapy client, we evaluate it across five distinct dimensions. None of them is search volume.
1. Patient Intent and Localization
The first question we ask: is this search coming from someone ready to book a session, or someone doing research?
A search for "EMDR therapist in Denver, CO" and a search for "What is EMDR?" both mention EMDR. One is a researcher who heard about a modality from a friend. The other has already decided they want it and is now finding someone to deliver it. The revenue difference between those two intents is not small.
We weight booking intent heavily, and we distinguish between several sub-types that matter for private practices:
- Local booking intent: "Trauma therapist in city," "specialty therapy near me" — highly valuable, relatively winnable
- Out-of-network private pay intent: "Private pay anxiety therapist," "out-of-pocket online trauma therapy" — these attract patients with high lifetime value who bypass insurance entirely, making them among the most strategically important targets for a practice
- Niche population search: "Therapist for first responders," "anxiety therapy for tech professionals" — lower volume, dramatically lower competition, very high conversion because the match is explicit
We map every content target to its intent type before anything else, because intent determines whether ranking actually connects to revenue.
2. Clinical Business Value
The second question: if someone finds this page and books an appointment, what is that patient worth to the practice?
Not all services are equal from a business perspective. A comprehensive neuropsychological evaluation, a long-term psychoanalytic engagement, or an executive coaching relationship represents fundamentally different lifetime value than a single intake session. Content should reflect these differences.
We map content targets to service tiers and deprioritize content that drives inquiries for low-margin, highly saturated, or capacity-constrained services — even when those keywords rank quickly. It's a common mistake to celebrate traffic from a content piece that keeps bringing in inquiries for a group therapy program the practice is already full on, while the individual intensive trauma work the therapist actually wants to fill goes unaddressed in the content strategy.
3. The E-E-A-T Authority Gap
The third question: what does the current search result page look like — and can a credentialed clinician realistically win here?
Google's E-E-A-T framework — Experience, Expertise, Authoritativeness, Trustworthiness — rewards demonstrably qualified authors in YMYL spaces. The key insight is that E-E-A-T is evaluated relative to what is already ranking, not against some absolute standard.
We evaluate the competitive market at the SERP level before recommending anything, and we map each opportunity across a simple continuum:
One end: A SERP dominated by generic directory listings (Psychology Today profiles, Yelp pages, local aggregators). These have essentially zero clinical E-E-A-T signal. A licensed therapist with a well-authored, specific page has a genuine structural advantage over them.
Other end: A SERP dominated by Mayo Clinic, the National Alliance on Mental Illness, and academic medical centers. These institutions have decades of established E-E-A-T signals in mental health. A local practice cannot close that gap on a general condition definition page, and trying to is a waste of budget.
The goal is to find and target the substantial middle ground where a credentialed clinician can differentiate on depth, specificity, and lived clinical expertise.
4. True Competition (Not Just Keyword Difficulty)
The fourth question: is this a battle a local private practice can actually win?
Standard keyword difficulty scores are useful inputs. They are not a sufficient analysis on their own, and this is where most keyword research leads practices into bad decisions.
The critical issue is that keyword difficulty scores are not linear in their real-world implications. The difference between a difficulty score of 15 and 25 is very different from the difference between 65 and 75. At the lower end, small differences reflect genuinely similar competitive environments. At the high end, small differences in reported difficulty can translate to large gaps in the actual effort required to rank. Domains with limited authority may find 70+ effectively unwinnable regardless of content quality.
We apply a non-linear competition model that aggressively rewards genuinely low-competition opportunities and effectively disqualifies high-difficulty targets, rather than treating competition as a flat scale. Only pick battles you are structurally positioned to win.
For a new or mid-authority domain, this often means targeting content with difficulty scores in ranges that most agencies would consider "too small to bother with." For mental health content, that assessment is often exactly wrong.
5. Execution Ease and Compliance Risk
The fifth question: can the clinician write this authentically, and does it carry compliance risk?
A therapist who specializes in trauma and works with first responders can write a deeply authoritative, experiential page on that topic from lived daily clinical practice. They cannot easily write a page that meets Google's E-E-A-T bar on general neuroscience, cognitive architecture, or psychiatric medication interactions. The former draws on authentic expertise. The latter requires heavy secondary research that produces content Google can distinguish from the work of someone who actually knows the subject.
We factor in the natural expertise match between the clinician and the topic, because content anchored in genuine clinical experience outperforms content constructed from sources. When Google evaluates E-E-A-T, depth that can only come from clinical practice is a differentiating signal — one that no amount of secondary research can replicate.
We also flag HIPAA and compliance friction upfront. Certain topics, particularly anything involving testimonials, specific outcomes, or clinical case patterns, require legal review before publication, or cannot be published in certain forms at all. Knowing this before a piece enters the workflow prevents wasted effort and protects the practice.
Hitting the SERP Wall
A content target can score well across all five dimensions and still be a poor investment if the SERP itself is structurally designed to suppress organic clicks.
We evaluate each target for three specific risk conditions before finalizing any recommendation:
AI Overview Dominance: For informational queries where Google is answering the question directly in the SERP, even a well-executed top-ranking page captures a fraction of the clicks it would otherwise attract.
Crisis Intervention Features: Queries touching acute mental health crises trigger mandatory SERP insertions. The 988 Lifeline box, safe messaging resource prompts, and similar features. These occupy above-the-fold real estate regardless of organic rankings. A page that ranks #1 below a crisis feature captures minimal traffic.
Knowledge Panel Saturation: Branded condition searches such as "depression," "PTSD," "OCD," "bipolar disorder", often trigger medical knowledge panels that dominate visual attention. These panels aggregate information from Google's own knowledge graph, leaving very little click-through intent for organic results even when the practice ranks well.
When any of these conditions are present, we reclassify even high-scoring targets as poor investments and redirect the same effort toward cleaner SERPs where organic rankings translate directly to patient inquiries.
This is why we systematically steer clients away from "What is condition" content. Not because it can't rank, but because ranking doesn't reliably translate to bookings in these SERP environments.
A Tale of Two Topics
The framework makes more sense in practice. Here are two content ideas that look similar on the surface, and why our evaluation produces completely different recommendations for each.
Topic A: What Is Depression?
This is the content idea that feels right to every therapist who first thinks about their blog strategy. High search volume, clear clinical relevance, easy to write.
Walk through the five dimensions:
- Intent: Entirely informational, no booking signal, no geographic component. This is research traffic, not patient acquisition traffic.
- Business Value: If someone books a session tracing back to this page, they almost certainly searched for something more specific before calling. The "What Is Depression?" page gets the traffic but not the bookings.
- Authority Gap: Mayo Clinic, the NIH, WebMD, and Healthline have owned this SERP for years. The authority gap is not closable for a local practice on a timescale that justifies the investment.
- True Competition: Effectively unwinnable for a domain with limited authority.
- Execution: High friction — to produce differentiated content here, the clinician would need to match the citational rigor of medical publishers. The result is usually content that reads like a summary of sources, not a demonstration of clinical expertise.
- SERP Risk: AI Overview almost certainly present. Potential knowledge panel. Possibly safe messaging features depending on the query variant.
Verdict: Very high volume. Near-zero practical value for patient acquisition. A content budget trap.
Topic B: Anxiety Therapy for Tech Professionals in [City]
Low search volume. Extremely specific. On the surface, it looks like a waste of time.
Walk through the same dimensions:
- Intent: High niche transactional intent. Someone searching this exact phrase is identifying themselves, naming their problem, and actively seeking a solution. They are close to booking.
- Business Value: Tech professionals frequently carry high-quality insurance, have disposable income for private pay, and tend toward long-term therapeutic engagement. This population represents high lifetime value.
- Authority Gap: Psychology Today has a profile page for the city, but not for this specific population niche. National publishers have nothing meaningfully targeted here. A therapist who works with this population regularly has an unambiguous E-E-A-T advantage.
- True Competition: Low difficulty — the specificity of the niche reduces competition to a handful of relevant pages, at most.
- Execution: If the clinician works with tech professionals regularly, they can write this page from authentic clinical experience in a few hours, and the result will read like genuine expertise, because it is.
- SERP Risk: Clean SERP. No crisis intervention box, no AI Overview, no knowledge panel. Organic rankings translate directly to clicks.
Verdict: Low search volume. Exceptional practical value. Exactly the kind of content that books patients.
The practice that writes Topic B consistently will outperform the one writing Topic A. Not because of SEO tricks, but because every page is engineered to connect the right patient, at the right moment, with a clinician who can actually help them.
What This Means for Your Practice
The question you ask at the start of a content strategy determines every piece that follows. Most practices start with "what are the highest-traffic keywords in my specialty?" and end up with a blog full of content competing against institutions they cannot beat, on topics that don't convert even when they rank.
The question that actually leads to patient acquisition is narrower: what are the searches where your specific clinical background creates an advantage, in SERP environments where ranking translates directly to calls?
This is the process behind every content recommendation Koppla makes. If you want to know how your current topics would score across these five dimensions, reach out or explore KopplaHQ. We'll run your existing content calendar through the framework and show you exactly where it's leaving patients on the table.